
In March 2021, India was hit by a devastating second COVID wave, resulting in multiple government lockdowns. Many of our team members were personally affected. As a result, we had to put our on-ground activities on hold for a few weeks. We quickly devised an emergency response to support the government and communities we were engaged with, to combat the pandemic in rural Madhya Pradesh. Our guiding principle was to emphasize prevention at the village level.
We adapted our interventions to ensure improved identification and tracking of high-risk COVID populations (e.g., elderly people, pregnant women, and people with co-morbidities). We supported the government by monitoring and supervising the response efforts. Additionally, we worked on ways to ensure the continuity of critical maternal and child health services.
We leveraged our grassroots knowledge of the health system and put together a three-pronged COVID-response plan
Bridge essential supply gaps
We provided frontline healthcare workers and staff at facilities personal safety kits and necessary screening tools, such as masks, gloves, sanitizers, and infrared thermometers and oximeters.
Build capacity
We equipped frontline workers and health staff with COVID knowledge and skills (COVID-response protocols, safety practices, use of screening equipment, effective counselling).
Vaccination mobilization
We raised awareness and created demand in rural communities on COVID prevention, testing, and vaccination with the help of educational materials and counselling.
Our COVID-response in 2021 covered
Our COVID response in 2021 covered approximately 35,000 frontline health workers and staff across about 6,800 villages, benefiting a population of roughly 11 million people across the six districts in Madhya Pradesh where we were working. Nearly 1.9 million units of safety and screening supplies were distributed. The district and state governments highly appreciated our support, and many of our team members received letters of recognition.





AAA Platform for COVID
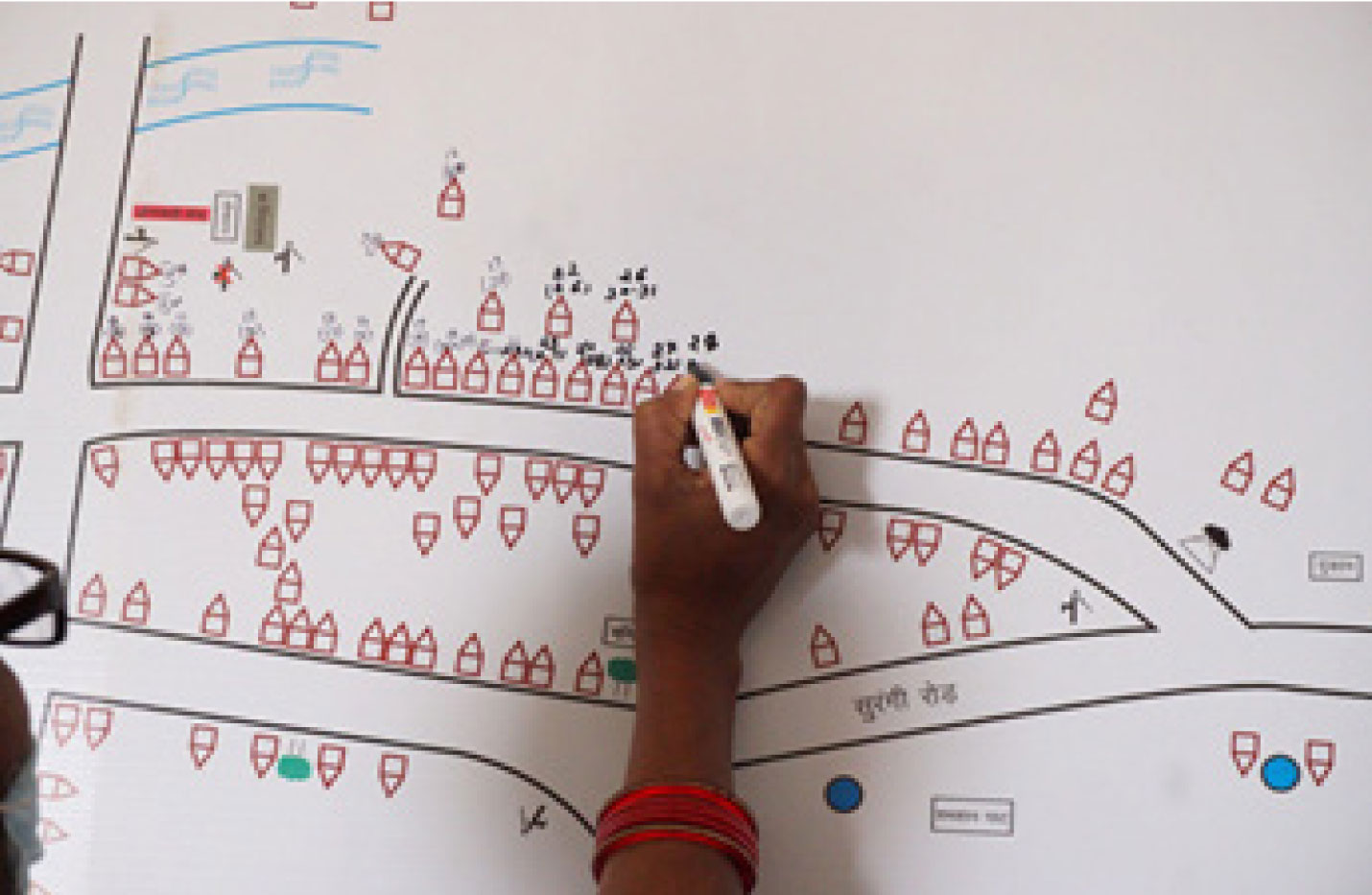
The AAA platform brings the three frontline health workers (ANM, ASHA, and Anganwadi Worker) on a collaborative data-sharing platform. This helps them create individual household-level village maps, micro-plan work to focus on the highest-risk mothers and children and conduct regular meetings to review each other’s work.
Our discussions with frontline workers and district administrators revealed a need for increased data sharing and collaboration for the various COVID-related tasks they were assigned. We modified the solution to identify, monitor, and timely manage individuals and households at high risk of contracting and carrying COVID (e.g., infants, pregnant women, migrants, elders, and people with comorbidities).
Using the village maps that were originally created to track the highest at-risk pregnant women, the frontline workers now started marking households with various high-risk codes for COVID (e.g., M-In for migrants who have returned to the village, 3D for women in their final trimester of pregnancy, 60+ for the elderly population), and collaboratively plan targeted efforts for these groups.
Pregnant women in their final trimesters require special counseling and monitoring to prepare them for safe institutional delivery. Assigning a COVID hospital to an asymptomatic pregnant woman and vice versa can be disastrous for the mother, child, and other patients in the facility. The AAA platform enables collaborative identification and monitoring of women for COVID symptoms. Using the village map, the AAA can also track out-of-hospital women and advise them on the necessary precautions.
Such joint action using the AAA platform’s simple innovations can save the lives of numerous mothers and newborns.


Maternal and child health during COVID
While it was necessary to contain the pandemic, the nationwide lockdown severely impacted critical maternal and child health services, resulting in a massive backlog of pending routine immunizations for children, ante-natal check-ups for pregnant women, growth monitoring for children, and other essential healthcare services. The omission of such services has the potential to significantly impact metrics such as infant mortality, maternal mortality, and child malnutrition levels – issues with which India has already been grappling for years.
We worked tirelessly to ensure the full resumption of all maternal and child health services in our intervention areas while adhering strictly to the COVID safety protocols.
Most of these health services are primarily delivered through monthly Village Health and Nutrition Days (VHND) in every village in rural India. VHNDs are led by the ANM (who typically manages four to five villages) and supported by the village’s ASHA and Anganwadi workers.
Our work ensured proper VHNDs happened across villages through two key initiatives-
VHND
Checklist
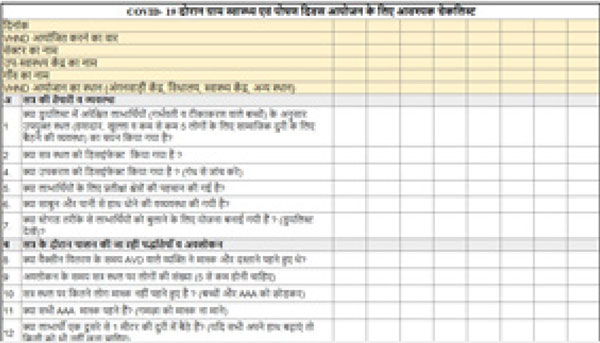
We created a comprehensive checklist for conducting a VHND, which frontline workers and government supervisors could use. It ensured safety by checking for site preparation (e.g., handwashing facilities, ventilation, social distancing measures) and correct practices that needed to be followed.
In one of the districts we work in, the district administration officially issued the checklist, and it was scaled even in geographical areas we don’t yet have a direct presence in.
On-site capacity
building

Our program officers visited different villages on VHNDs. We used these visits to handhold frontline workers to ensure proper site preparation and practice COVID-19 protocols – for example, maintaining social distancing, appropriate use of masks, hand-washing, staggering presence of beneficiaries, etc. We also guided them on how to plan additional efforts to cover beneficiaries missed during the lockdown.

Capacity building to combat COVID
Frontline health workers have been tasked with critical COVID work such as; spreading awareness on prevention and control, identifying potential cases, addressing misconception and stigma, supporting contact tracing, and quarantine implementation. The success of the government’s COVID efforts hinged largely on frontline workers’ capabilities to perform these tasks well. However, given the novelty of the virus, ensuring timely and adequate knowledge was a challenge
Our field observations highlighted several areas that required focused attention. We trained different cadres of health workers through virtual meetings to mitigate the knowledge and skill gaps, focussing on the priority areas identified.

Snapshot of a virtual capacity-building training of frontline health workers on COVID,
being conducted by The Antara Foundation program team
Key topics covered by TAF included –
- Understanding the symptoms of the virus
- Prevention and control of the virus
- Special care required for high-risk groups (e.g., elderly, pregnant women)
- Management of symptomatic cases; contact tracing process
- Protocols for home quarantine
- Tackling stigma associated with the virus, including myths and misconceptions
- Correct detection procedures – temperature measurement using infra-red thermometers, and oxygen saturation measurement through pulse oximeters
- Frontline worker safety protocols while handling suspected cases

Capacity building to tackle stigma
Supporting government in filling the critical knowledge gaps of frontline workers on tackling stigma
Myths and misconceptions about COVID often lead to stigma against affected patients, health workers, migrant workers, and so on. Marking households with quarantined patients can also have a social stigma attached. This leads to cases being concealed and reported late, making response efforts more difficult. We trained frontline workers on managing stigma in their populations – for example, avoiding using terms like “suspected case” or “victims,” sensitizing people correctly, and so on.



Monitoring and supervision
Robust monitoring and reporting of data is critical for effective planning and implementation of the COVID response.
We supported the district authorities by creating comprehensive and easy-to-use monitoring formats for different COVID response activities. Below are two examples:
Below are two examples:
Migrant tracker
We incorporated a migrant tracking format as part of the new ASHA diary (designed through TAF support and scaled up across Madhya Pradesh). In some areas where we work, we supported the district administration in enhancing their migration tracking formats.
Screening format
We supported district administrations in Madhya Pradesh by creating monitoring formats for frontline workers for the 15-day “Kill Corona” campaign launched across the state in July 2020. The campaign involved active fever screening and appropriate management of symptomatic cases across the district.