
TAF believes that the community is not a beneficiary but a partner. Our integrated approach places women at the centre of health solutions, recognizing their unique ability to identify and resolve the issues they face.

We work through three powerful models:
PLA model

Faliya volunteer model
MEG model
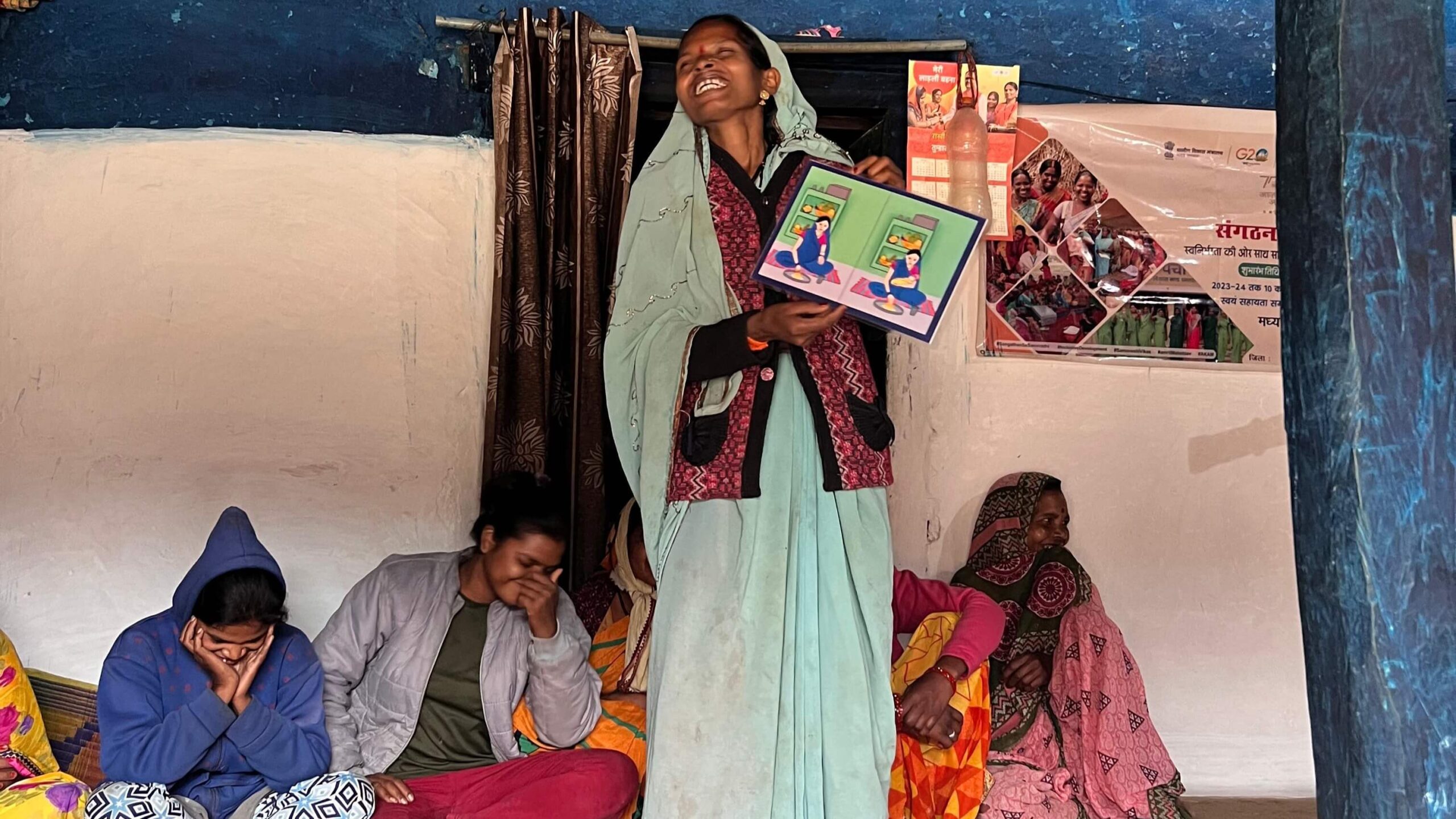
In partnership with Ekjut, the PLA model uses adult learning methods like picture cards and games to promote awareness and encourage health-seeking behaviour. Women evolve from Learners to Seekers, Activists, and ultimately Partners.
In hilly and dispersed tribal regions, villages are scattered into clusters called faliyas. To bring services closer to these remote pockets, TAF supports a faliya-based volunteer system. Young local volunteers from each faliya attend monthly VHND meetings, support high-risk cases, and work closely with frontline workers.
In addition to their role in case identification and follow-up, these volunteers help organise Village Health and Nutrition Days, not just at the village level, but also smaller, more accessible VHNDs within their own faliyas. This makes it easier for women and children in distant hamlets to access essential health services.
Results in Barwani showed a 77% decline in home births.
Mothers Enablers Groups create safe spaces for pregnant and lactating women to share, learn, and lead. These groups build peer networks where women discuss health challenges, gain clarity on government entitlements, and support one another through the critical first 1,000 days of motherhood. Facilitated by trained community members and frontline workers, MEGs foster a sense of solidarity and confidence among women, enabling them to become informed decision-makers for their families’ health.

