 Life in rural India
Life in rural IndiaAntara Foundation works at the grassroots of public health delivery with some of the most marginalized communities in rural India. What is “community” for us? First, government frontline health workers, drawn mostly from local communities – the nurse-midwife (or ANM), the ASHA worker (village health mobilizer) and the anganwadi worker (nutrition caretaker). The second, the larger community of village populations, with our interventions focused on pregnant women, lactating mothers, newborns, and children. This article introduces you to the latter, that is, our end beneficiaries, and highlights various aspects of their lives.
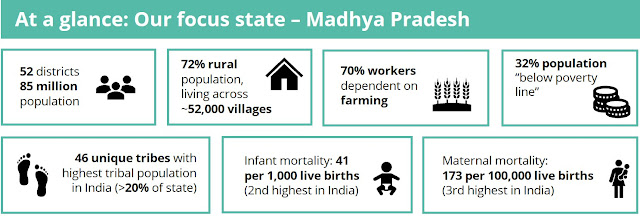
Where we work
We work in the state of Madhya Pradesh, India’s fifth most populous state (~85m people) and second largest in expanse. Located at the heart of India (“Madhya” means central in Hindi), the state’s terrain is characterized by low mountain ranges, extensive plateaus and river valleys and is home to ten national parks.
Large areas within the state are characterized by extreme poverty, inadequate infrastructure and development, challenging terrain, and consequently poor socio-economic indicators. In three of our districts, almost 40% of the communities are tribal populations. The Indian government designates populations as “tribal” based on factors such as primitive traits, distinct culture, geographical isolation, shyness, and backwardness. Historically disadvantaged and discriminated against, tribal communities have significantly worse socio-economic metrics.

See what life is like in Madhua Dhana, a typical central Indian village we work in.
Drag the video around for a 360-degree immersive experience.
Click to view video on YouTube: Life in rural India (5 mins)
Health situation
Amidst its diverse cultures and beautiful landscapes, Madhya Pradesh also has some of the worst health outcomes in the country. Tribal populations are extremely heterogenous, each with diverse cultures and distinct social norms. Several of these norms are based around the critical 1,000 days between conception and age-2 of a child, and are severely detrimental to health. Some stark examples include – giving inadequate food to pregnant women to reduce the baby’s size, spiritual healing for severe labor pain, discarding colostrum (nutritious first breast milk, critical for the newborn), and conducting rituals to heal malnourished children. These communities, therefore, account for a disproportionate share of the health burden.
Access to proper healthcare is also challenging. There are issues of livelihood – the average monthly income per agricultural household is as low as INR 8,300 ($110), with many households surviving on daily wages. Access to health facilities is problematic, with poor public transport and lack of roads in many villages. Travelling to a health institute for check-up, or treatment kilometers away means losing out on a day’s wages. Many a time, health is overshadowed by issues like water, food, and gender norms.
The issues are exacerbated due to the intersectionality of rurality, poverty, traditional belief systems and adverse socio-cultural norms. Rural women at the intersection of these factors become particularly more vulnerable, because they are disempowered to have a say on their health and the health of their children.
Working with and through our communities
We strongly believe that the best solutions to complex health problems come from those closest to, and most affected by the issues. Listening to and learning from our village communities is therefore a crucial element of our program design. We work in some of the remotest villages, often reached only by foot.
Our teams regularly visit these communities to meet and learn from pregnant and lactating women, frontline health workers, broader women’s groups, and other village change agents such as elected representatives and adolescent girls. This is key for us to understand health-related challenges better, find ways to overcome health barriers and create impactful and lasting solutions.


View larger images in the album here