 The promise of virtual training platforms in grassroots health interventions
The promise of virtual training platforms in grassroots health interventionsA silver lining during the COVID-19 pandemic has been the dramatic rise of technology as an enabler for service delivery. Virtual meeting tools and software have transformed sectors – for example, tele-medicine in health, virtual schools in education and digital marketplaces for agriculture. In this article, we talk about the promise of virtual platforms to deliver maternal and child health interventions, highlighting three innovations from our work across remote and rural villages of India.
The Antara Foundation (TAF) strengthens health systems to improve maternal and child health. Our programs train community health workers (CHWs), make data-sharing more effective, build supervisory capacity and improve health facilities. The lockdowns and safety measures imposed due to COVID-19 caused a slowdown in several program activities due to travel restrictions, limitations on holding large group meetings and the unavailability of health workers because of additional COVID-response duties.
To address this, our team redesigned elements of the program to deliver select activities remotely, to supplement in-person trainings and maintain continuity of our interventions.
1. Virtual capacity building to improve essential MCHN knowledge
Our capacity building work improves knowledge and skills of CHWs on essential maternal, child health and nutrition themes. Detailed assessments are carried out to identify knowledge gaps and inform the curriculum. The format involves a mix of group trainings and on-site handholding for weaker staff. During the pandemic, short virtual training packages were designed, with visually engaging modules and interactive content such as handouts and quizzes. Feedback from the CHWs was very encouraging.
Such targeted virtual sessions are now a core part of our capacity building approach to supplement in-person trainings. Their success stems from the following: first, virtual sessions can be more personalized, targeted and interactive; second, sessions can be scheduled with more flexibility to accommodate health workers’ busy schedules; third, they require fewer resources compared to classroom trainings; and they have the potential to transform into self-sustaining peer learning groups in the future.
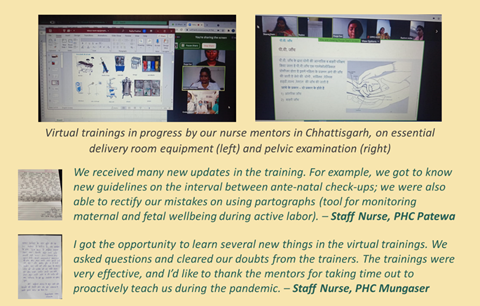
2. Virtual nurse mentoring for government birthing nurses
TAF’s nurse mentoring solution plugs critical knowledge and skill gaps in nurses who conduct deliveries in government labor rooms. The comprehensive training package covers 48 modules across seven key themes and is delivered through a series of classroom sessions and live demonstrations.
In our Chhattisgarh program, special virtual mentoring sessions were planned during COVID lockdowns to refresh concepts from previous trainings and discuss new modules. The format incorporated interactive case-based discussions, with pre and post online quizzes to increase engagement and ensure retention. The initiative proved immensely useful for the nurses to keep up to date and remain connected to their mentors and peers.
3. Virtual AAA meetings
The AAA [Note 1] Platform is TAF’s flagship solution that brings the three community health workers in each village on a collaborative data-sharing platform. The AAA together create a detailed household level village map and mark critical beneficiaries with different colored bindis. Each month, they meet to pinpoint the highest-risk mothers and children, micro-plan service delivery, and review each other’s work.
In Chhindwara district, village maps have been created and installed in all ~900 villages of our focus blocks. Our team is now training the AAA to conduct effective ‘AAA meetings’. During the lockdown, our team ran virtual AAA meetings in select villages to help AAA identify high-risk beneficiaries, develop follow-up plans, cross-check their data reporting, check availability of medicines and supplies and recap essential knowledge.
The virtual sessions involved collaborative discussion and data analysis. Several critical action items were identified and promptly managed (e.g., anemic pregnant women requiring urgent blood transfusion or iron sucrose, requirement for antibiotics, iron and calcium tablets, vaccines).

We are enthusiastic about the early results from these targeted pilots. The willingness of health officials and CHWs to take to technology is encouraging. However, factors like device affordability, internet connectivity and basic IT skills are barriers still facing a large section of rural India. Until this ‘digital divide’ remains, scalability of purely virtual solutions will be a challenge. Meanwhile, we believe hybrid is the way to go, where technology supports and strengthens in-person grassroots health innovations.
Our previous work in Rajasthan has shown the wonders technology can achieve. When our ‘AAA Platform’ was taken up by the government for state-wide scale-up across Rajasthan’s 46,000 villages, more than 125,000 CHWs were oriented through video conferencing in a span of just a few weeks! Pilots of our ‘Integrated AAA App’ (mobile App for real-time data sharing between CHWs) showed a significant increase in the identification of high-risk mothers and children as compared to the offline process.
The possibilities are enormous, and we hope to increasingly harness the power of technology to further our mission.
Note1: AAA stands for ANM, ASHA and Anganwadi Worker – the three community workers who deliver health and nutrition services in each village in India