 Closer to Community, Closer to Better Outcomes
Closer to Community, Closer to Better OutcomesOn our visits to the field, community health workers (CHWs) often tell us, “When you join us for a field visit, everyone listens to what we say. But once you leave, we’re left on our own and nobody pays any attention to us.”
While supervisors within the system have been a constant support to CHWs, their experiences also reflect a recurring reality across many villages. CHWs often feel the absence of a support mechanism in their everyday work, making it difficult to keep up their motivation over time.
To improve health outcomes, and sustain them, CHWs need to remain consistently engaged in their roles. This becomes challenging amid the many constraints they face, particularly without collective, locally rooted support.
Those who are readily present within a village are members of the community itself. Despite the absence of formal responsibility, they remain deeply invested in the health and wellbeing of their families and neighbours. When communities are intentionally involved in supporting CHWs, a sense of shared ownership begins to take root, strengthening trust and increasing the uptake of institutional care.
A core part of our work at The Antara Foundation (TAF) involves strengthening the capacity and outreach of the public healthcare system by training and bringing together Anganwadi Workers, ASHAs and ANMs (AAAs). We also train supervisors to mentor and guide CHWs across intervention areas. However, such support cannot always be physically present. While system strengthening is essential, meaningful change also requires communities to be a part of it – empowered as active participants in seeking quality care. – empowered as active participants in seeking quality care.
This year, our AAA platform is evolving into the Community + AAA (CAAA) platform. Under the new approach, an active community member (ACM) participates in the village-level review and planning meetings (baithak) along with CHWs to help identify and resolve everyday challenges. In some cases, ACMs volunteer to ‘adopt a bindi’ – figuratively adopting a pregnant woman whom they will regularly visit and motivate to seek public healthcare services. Volunteers live in the same cluster, and hence take one round, almost every day, to their house – sometimes to check if woman consumed supplements on time or if she needs any further support reaching out to CHWs. The village map is a visual tool we provide across our program areas. CHWs put coloured bindis on the houses where their service recipients reside. This helps them plan their home visits and get a bird’s-eye view of overall service requirements of their village.
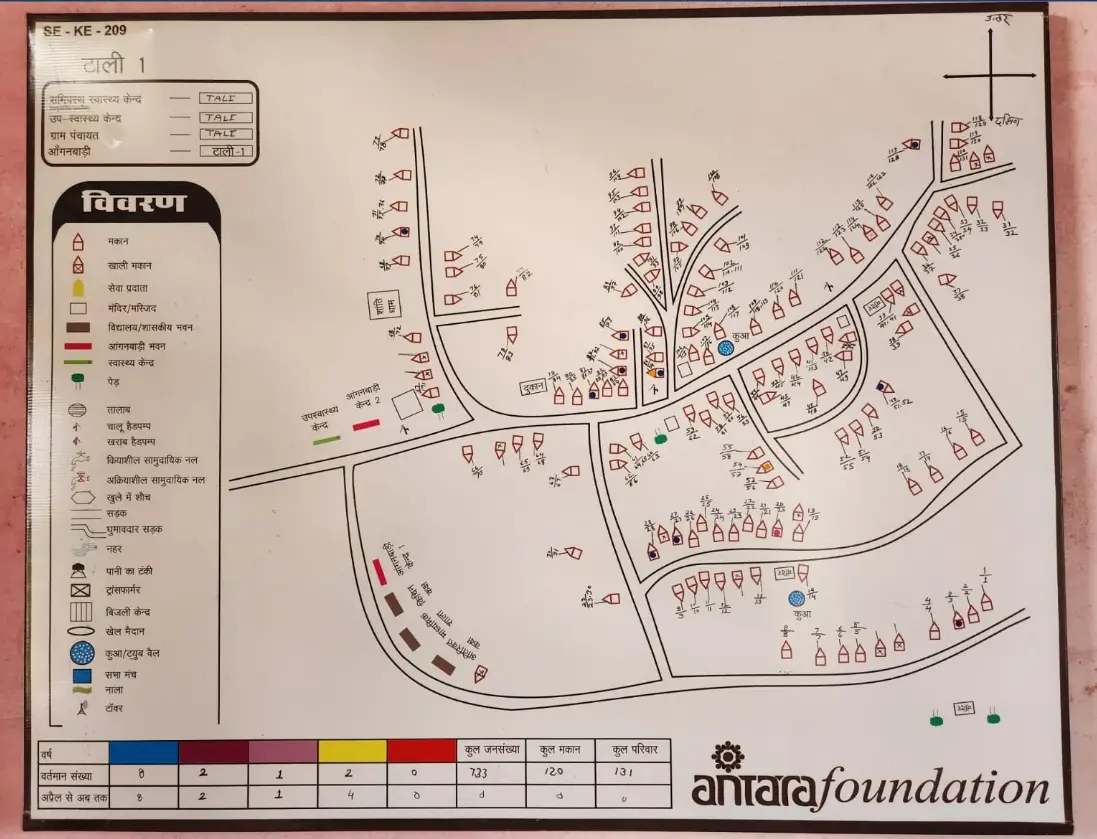
The village map is a visual planning tool for CHWs to provide health services to mothers and children.
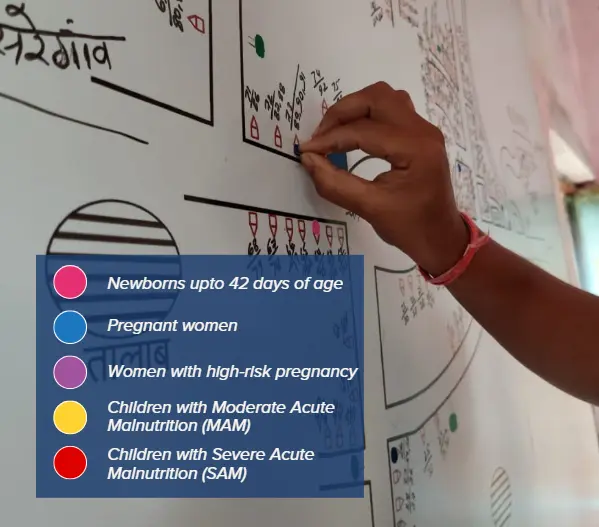
The CHWs stick different coloured bindis that represent their key service recipients onto the village map, giving them an overview of the village.
Across our interventions, TAF is moving towards deeper community collaboration, involving mothers, children, and families in shaping how healthcare is delivered and received. Communities engage through CAAA meetings, volunteer opportunities, mothers and enablers groups (MEG), community conversations, and Participatory Learning and Action (PLA) meetings. Through these engagements, CHWs experience a stronger sense of shared responsibility, making their work feel more supported and manageable. Families, too, are more willing to accept services when trusted community members are visibly involved. We also recruit facilitators from the same community, who enable these engagements and help us identify community volunteers motivated to drive change.

Ramayani didi participating in CAAA meeting, along with other volunteers
One such example is Ramayani didi, a community champion who began advocating for healthy pregnancy after learning about its importance through TAF’s meetings. She was pregnant herself when she attended her first MEG meeting, where adolescents, pregnant and lactating women, and their caregivers come together to discuss maternal health challenges in the village. During the meeting, CHWs explained the services available through the monthly Village Health, Sanitation and Nutrition Day (VHSND) at the Gram Aarogya Kendra. They also shared information about the CAAA meeting held immediately after the VHSND event, a platform for community to help CHWs tackle the challenges.
Ramayani didi actively participated throughout the meeting – sharing her concerns, asking about services and giving examples from the village. Recognising her engagement, the facilitator identified her as a potential volunteer and invited her to join the CAAA meeting. It was here that Ramayani didi learnt about Kamala*, a pregnant woman with high blood pressure and mild anaemia.
Distressed to hear that routine counselling by the AAA had not yielded effective results, Ramayani didi took it upon herself to support Kamala. She began visiting Kamala regularly to monitor her diet and supplement intake. Over time, Kamala started regularly accompanying Ramayani didi to antenatal check-ups (ANC) at the Anganwadi Centre, and her haemoglobin levels improved. While AAAs are mostly from the same village, their residence could be far or their communities might differ. At the village level, these differences can create huge communication gaps between them. In such cases, support like Ramayani didi’s is necessary to bridge trust. Ramayani didi did not only act as an ambassador of public health services, but also a trusted support for CHWs.
Another active community member, Jyoti Nagle, who volunteered to support Payal* with her high-risk pregnancy shared her determination: “Next time, I want to replace her purple bindi with a blue one on the map.”
TAF’s community-integrated models aim to create a holistic ecosystem of interventions, where improvements in service quality are matched by greater community willingness to seek care. Thus far, the burden was on CHWs, who acted as the only bridge between public healthcare system and the community. However today, community champions like Ramayani didi are emerging as a crucial link for CHWs in translating their village level plan into action.
To this date, TAF has facilitated many community-level meetings and conducted over 8,000 Participatory Learning and Action (PLA) meetings, mobilising more than 150,000 community members across villages. Many active community members emerge from these meetings who initiate conversations about women’s health within their families and communities. These conversations are drivers of empowering change for mothers.
Sustaining this momentum will require motivation to build an integrated public healthcare system, one that recognises communities not just as beneficiaries, but as essential partners in care.

Ramayani Didi sitting in CAAA meeting with other two volunteers from village