The Accredited Social Health Activist (ASHA), Anganwadi Worker (AWW), the Auxiliary Nurse Midwife (ANM) and the Community Health Officer (CHO) are the first line of public health service delivery for communities in rural India. They are responsible for delivering primary health care and nutritional services to pregnant women, mothers and children.




While these frontline workers function in the same areas to attain similar goals, they often don’t collaborate with each other. This leads to many beneficiaries being left out of receiving crucial health delivery services. Appointed by the MoHFW (Ministry of Health and Family Welfare), the ASHA acts as the village health mobiliser, facilitating the community in accessing proper health-related services and the ANM offers vaccination and health services for a Sub-Centre, which is normally a group of 4-5 villages. The AWW, appointed by the Integrated Child Development Scheme (ICDS), is in charge of nutrition and early childhood education and development of the children in the village.
Despite having a well-designed healthcare delivery mechanism, India’s maternal and child health and nutrition (MCHN) indicators continue to remain low. This is in part due to poor coordination between the frontline health workers, which results in these three women working individually despite operating in the same village and having the same goals and beneficiaries. As a result, when they run into a challenge at work, they often feel isolated and stuck.
The Antara Foundation’s flagship intervention, the AAA platform, brought all four parties together to work together as a team, to carry out their responsibilities more efficiently and plan, work and resolve health-related issues easily.

01
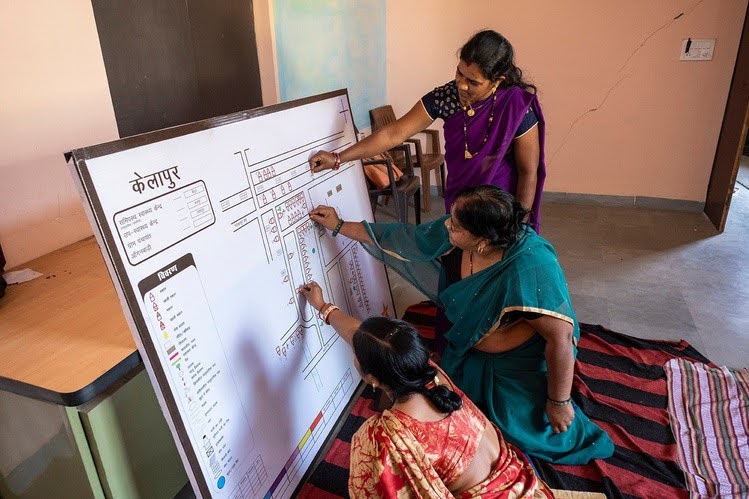
In this phase, the AAA creates a village map, a tool introduced by TAF for smart service delivery, with the help of the village community. As a result, there are no left out beneficiaries. They then number the houses on the map and mark the houses of high risk and other beneficiaries with bindis. This map acts as a common database, which they regularly keep updating in their meetings. It helps them to get a snapshot view of all the cases that they have to handle and plan their visits efficiently.
02
In this phase, they review, plan,and learnfrom each other during their AAA meeting which happens after every Village Health and Nutrition Day (VHND), which is held once a month.
The AAA platform helps the frontline workers in improving data accuracy and consistency across their registers, identifying and prioritizing high-risk beneficiaries and improving the quality of their service delivery through shared learnings.
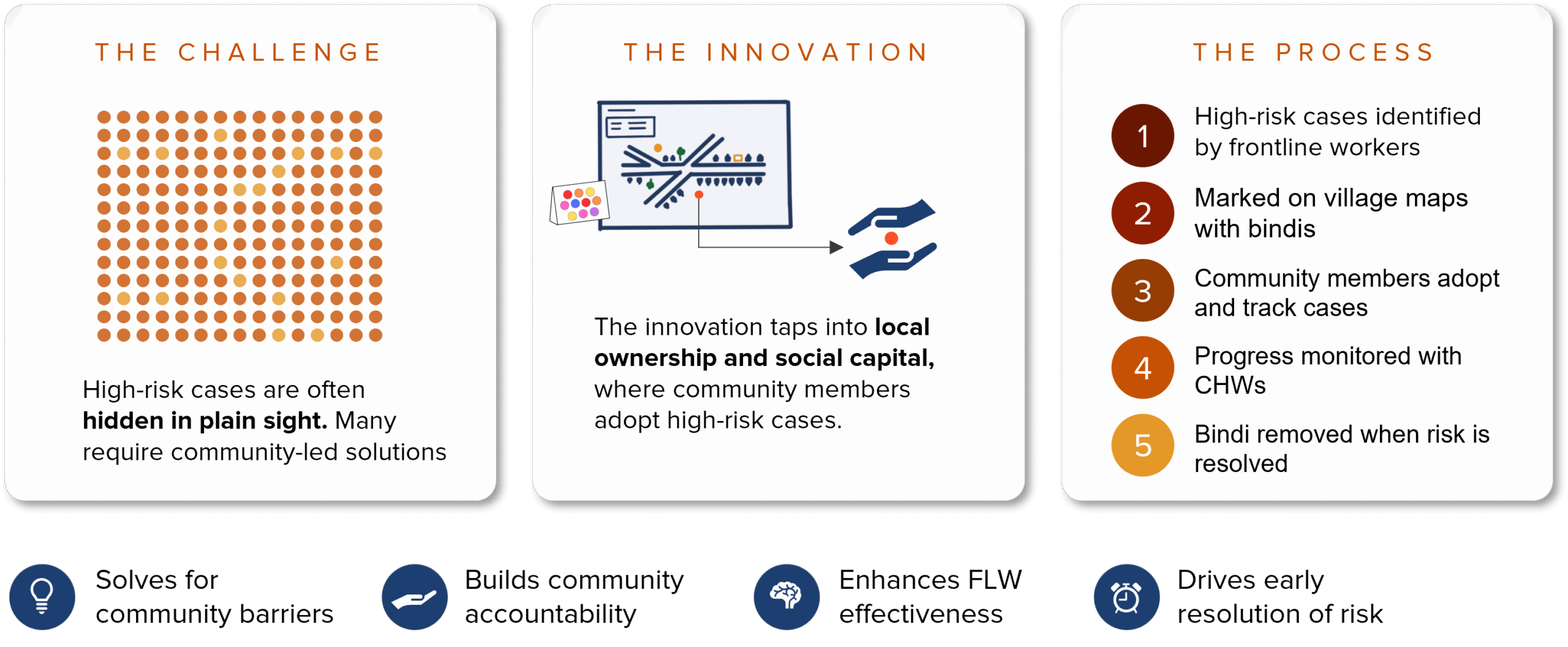
The Community-AAA (CAAA) platform strengthens the proven AAA Platform by integrating community ownership. In this approach, the three frontline workers (ASHA, Anganwadi worker, and ANM) come together every month to identify high-risk pregnancies, low-birth-weight newborns, and malnourished children, using coloured bindis on village maps.
Adopt a Bindi is an initiative under the broader CAAA platform. In this intervention, respected village women form a voluntary cadre of Active Community Leaders (ACLs) who attend AAA meetings, identify cases, and ensure that each high-risk case is personally supported by a community member. This approach not only strengthens follow-up care but also increases community ownership toward seeking timely healthcare. Critical cases are escalated to local authorities when needed. The goal is simple: no mother or child should fall through the cracks. The model, piloted in 83 villages in Chhindwara, is now being scaled to 800+ villages.
“Adopt a Bindi might sound innocuous, but it has the potential to be the most direct, fastest, and highestpayback intervention in our program.”